

Some data on active caseloads
Before beginning, note that David Siegel recently interviewed me:
https://www.youtube.com/watch?v=munQedJ7rSY
The following list is far from complete, but suggestive:
Countries with over 100 total reported cases, and none active:
Mauritius, Faeroe Islands
Countries with over 100 total reported cases, less than ten active:
Cambodia, Brunei, Montenegro, Trinidad
Countries with less than 100 reported active cases, falling rapidly:
Iceland, New Zealand, China, Hong Kong, Taiwan, Palestine (plus Montana, Alaska, Hawaii)
Countries with less than 200 reported active cases, falling rapidly:
Thailand, Luxembourg, Albania, Andorra
Countries with less than 1000 reported active cases, falling rapidly:
South Korea, Australia, Croatia, Lithuania, Tunisia
Countries with less than 2000 reported active cases, falling rapidly:
Switzerland, Austria, Denmark, Norway (probably, no hard data), Malaysia
Countries with less than 20,000 reported active cases, falling rapidly:
Germany, Japan, Ireland, Israel, Czechia
What can we infer from this list? Total caseloads in the US continue to rise (now over a million), although it’s starting to level off. Global totals also continue to rise. But there are many countries with fast falling caseloads, some approaching zero. And these countries are of all types: big & small, rich & poor, East & West, hot & cold, state capacity and state incompetence.
In a few weeks, almost all of these countries will have many fewer cases than they have right now. I’ll try to remember to revisit this list in mid-June. The world is dividing into two groups, the successful and the failed states. Sometimes (as in the USA) you have both types in the very same country.
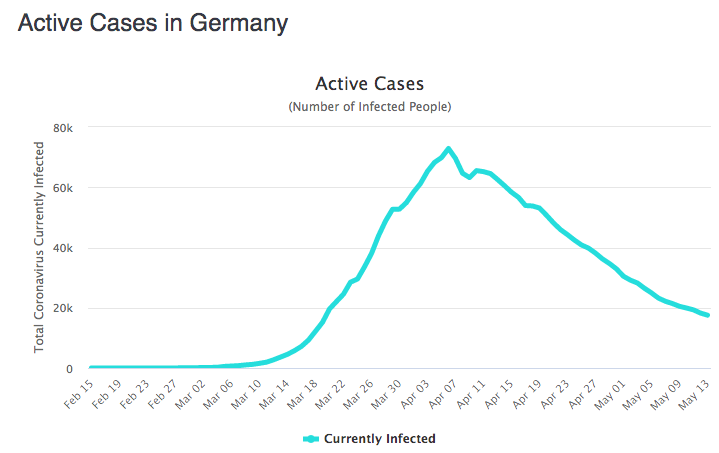
PS. Of all the countries on my list, Germany has by far the biggest active caseload. But even its active caseload graph has the characteristic shape:
PPS. Countries on this list continue to see declining active caseloads even when hit by secondary waves, as in South Korea.
Tags:
14. May 2020 at 22:33
Scott, somewhat off-topic question: do you have an opinion on moving conventional monetary policy from using very short term bonds to eg perpetual bonds?
That would be a way to side-step the whole zero lower bound issue without having to tackle the misconception heads on.
I guess the more general question: would monetary policy via buying and selling longer duration bonds work?
15. May 2020 at 00:30
Active case load seems to me to be at least a couple degrees removed from being a particularly useful statistic. Not only do countries vary widely in how much they’re testing, but also in the rate of change in how much they’re testing, and the standards that determine who gets tested (and the consistency of those standards across time). I would at least start though by dividing by the number of tests done in each country. (This my sound rather first-world elitist, but, absent more controlled studies or standard international protocols, I think there are likely serious differences between Switzerland and Tunisia in testing capacity, efficiency, and responsiveness to outbreaks, etc. that will impose differences between countries in the relationship between the actual number of cases and observed number).
15. May 2020 at 02:43
Scott,
The fact that you have left Vietnam off the list tells me you are using the wrong criteria.
No fatalities at all. No new domestic cases in over a month. (All the new cases are overseas Vietnamese who are being repatriated and going straight into quarantine.
The countries with low caseloads are not ALL types. They all either have had warm weather and/or universal neonatal BCG vaccination programs.
And again your characterization of “successful and failed” misses the mark. Caseloads appear to have very little to do with success or failure of either the government or society as a whole.
15. May 2020 at 04:05
Dtoh,
Singapore, warm, universal neonatal BCG vaccination, possibly the highest and most competent state capacity on the planet. Population 5.5 Mio, 26,000 cases, rising linearly for a good 6 weeks now. This after spending the first 2 months of the pandemic with very few cases due to effective and disciplined tracking, testing, and immediate isolation of every sick patient. Yes it is mostly affecting the worker’s dorms but they too come from countries with routine BCG vaccination (e.g. India, Bangladesh) and I doubt they use a/c a lot. What Scott is pointing out is the randomness in the whole process. There doesn’t seem to be a universal predictor on how this plays out. Luckily it seems that eventually, regardless of what you do or don’t do, there is a peak and then a linear decline, as there was fairly linear (not really exponential, except at the beginning) rise. And this decline happens much before anywhere near herd immunity is approached. What gives?
I’m much more surprised that some of the countries with the most extreme measures, such as Italy and Spain, have not really seen more radical declines commensurate with their desperate efforts.
15. May 2020 at 05:17
We will see in time. Seems to me Covid is never going away. This flu season in the US: 39 million flu illnesses, 400,000 hospitalizations and 24,000 deaths – including 162 children. Laboratory-confirmed influenza-associated hospitalizations (19,543). All this despite there being a vaccine,and proven treatments. In 2017 I got type A despite being vaccinated for type A – as I learned the vaccine can be as low as 40% effective.
15. May 2020 at 07:46
“Start Dates” ——which sometimes is when counting started, but likely a combo of both counting and when real disease showed up—-has been largely linked to decline “dates”. We are about 12-18 days behind Western Europe——so we should expect to see similar declines. Although Russia has a very late start date—-and approaching peak—-same with Brazil.
Taiwan and HongKong have less than .5 deaths per million. I believe they are honest in their attempts to count. I find this has not been explained in any way scientifically. The Atlantic tried to give a general cultural reason why for Hong Kong——but did not have much useful information. It surprises me we have not tried to answer that question. Japan——largest number of Chinese visitors in 2019—has only 5 Deaths per million (similar 5 per million in Singapore). I have to classify these As unanswered mysteries.
Only 2% of active cases (2.5mil) currently are considered very serious. It appears that we are approaching a global leveling (likely to decline it would seem within 2 months at the latest) of active cases——hence some leveling out death rates to be expected. Absent vaccine how low can that go?. Assuming it levels out at 2mil, with a 2% death rate and a 30 day “turnover” that is about 500,000 deaths per year. That seems low——But appears consistent with global trends of the Covid virus .500k-1mil Constant annual deaths globally seems plausible, perhaps conservative (not to put too fine a Ghoulish point on it, but we eventually start running out of older people at a faster rate than we increase them)
Many conjectures on whether lockdowns “work”—many more on whether danger to economy Itself causes deaths—-
We cannot argue that this experiment of ours is unprecedented——and we cannot argue that these diseases disappeared fast (although 1918 was horrific) doing “nothing”.
But we do not have to do “nothing”. But open ended lockdowns are going to destroy us—-at some point it is up to the “free market”——sooner rather than later.
15. May 2020 at 08:03
Matthias, We already buy and sell longer term bonds as a part of monetary policy. I have no objection to perpetual bonds, I just don’t see it as having much effect on monetary policy.
Mark, If the rapidly falling active caseloads were far off course it would show up in other data like fatalities. I do agree that there is huge underreporting due to lack of testing, I just don’t think it explains fast falling active caseloads.
dtoh, This was a list of countries where the active caseloads are either below 10 or falling fast. Vietnam is not such a country. it is highly successful in controlling the coronavirus, as you say, but this is not a list of highly successful countries. It is a list of countries highly successful at rapidly reducing active caseloads.
It’s also not a complete list, as I said in the intro.
I actually had Vietnam on my original list, then double checked its active caseloads, saw they were no longer falling, and took it off.
Matt, You said:
“We will see in time.”
Yes, in a few weeks. I made no predictions beyond two weeks. I am guessing that you assumed otherwise.
15. May 2020 at 08:11
Active cases is not a very good measure of anything:
* Every country is badly undercounting cases because so many are asymptomatic. I would argue the US is now testing better than some other countries, including France, UK — it’s positive rate is well below other countries. If death rate is 1%, then true count of cases is 5-10x where it appears to be, so just small adjustments in detection make a huge difference. Although lagged by 3-4 weeks, death rats are in the end a better measure of how a country is doing.
* Active cases depends on tracking recoveries. US is not systematically tracking these.
* Most important, all that really matters is death rates. Active cases – even symptomatic ones — in which a person stays home, has fever and recovers are not at all a problem. Should the state be trying to lower that? That kind of case is like the flu. It’s the deaths that make it different, so that’s what should be tracked. And death #’s also will be a proxy for how much hospitals are overwhelmed, since many of these serious cases also show up in the hospital.
* The US is high in # of deaths per million, higher than most countries, but there are definitely countries that have higher death #s per million — Sweden, UK, Italy, Spain, Frank, Belgium, Netherlands. And I think those numbers — at this point — most correctly represent how the US has done in this — worse than most but not the worst.
* Finally, we really do have to look regionally, both in the US and in other countries. It’s the outbreaks that really result in the huge death numbers. It’s very much a local disease. Of course, there is air travel that can spread it, that has been low for some time. So we have to ask, are the local governments responsible for these local outbreaks? Probably in some cases, yes, in some no. Until you really think through which layer of governments owns what responsibility, I think it’s a mistake to talk about failed states. It’s clear the mayor of NYC was very much downplaying this quite late and the biggest outbreak — by far — in the US was there. On the other hand, NY is also a dense place. But almost 50% of deaths in the US are basically the NY metropolitan area. How do we evaluate that?
15. May 2020 at 08:13
Scott, I was talking more generally and over a longer period of about 18-24 months.
15. May 2020 at 08:32
If 40% of the US population is high risk due to obesity vs. the 10-15% in most of the rest of the developed world, the US death rates could be interpreted as the most successful in the world.
Without clear and consistent definition and measurement, all the talk about success and failure just seems like mood affiliation and cheer-leading.
15. May 2020 at 08:44
“The world is dividing into two groups, the successful and the failed states. Sometimes (as in the USA) you have both types in the very same country.”
But you also say:
“But there are many countries with fast falling caseloads, some approaching zero. And these countries are of all types: big & small, rich & poor, East & West, hot & cold, state capacity and state incompetence.”
If state incompetence doesn’t move you from the category of successful state to failed state, wouldn’t it be more appropriate to say the world is dividing into two categories, lucky states and unlucky states? And if it really is just luck, then doesn’t that suggest that things will even out in the long run, rather than divide further?
15. May 2020 at 08:51
Thailand was clogged with Chinese tourists and Bangkok is as crowded as anywhere, lots of public transit.
56 C19 deaths in a pop of 70 million in Thailand. Lots of crowded housing in Thailand, and people are not sticklers for rules.
US pop 330 mil and nearly 90,000 dead.
Makes no rhyme or reason.
15. May 2020 at 09:52
@Benjamin Cole
Seems like the most obvious explanation would be that Thailand is simply not counting and/or reporting this information.
15. May 2020 at 10:08
The countries worse hit as measured by recorded deaths per million of population are mostly rich Western European countries (Belgium, Spain, Italy, UK, France, Sweden and Netherlands). These countries have high GDP and excellent health services. The US which is a bit richer and spends more on health (while currently doing slightly better) will probably end up somewhere in the same ballpark as these rich Western European countries. Meanwhile almost all other countries – poor counties,East European Countries, Asian countries, Southern hemisphere countries (even those that are quite similar in most regards to the US and Western Europe) – are apparently doing much better.
Not sure what this tells us but I’m pretty sure there is more going on here than meets the eye.
15. May 2020 at 13:23
US had very limited testing capacity early in its epidemic, which makes their “curve” appear less flat than it really is, presumably.
15. May 2020 at 13:34
@Benjamin,
Hong Kong also has crowded living conditions, one or two people, from China, yet has had fewer deaths than Thailand.
Maybe the large scale social distancing in place in Thailand has something to do with the low number of deaths. But hey what do I know.
15. May 2020 at 16:41
Scott,
A few comments.
Vietnam – To remind you of your post where you said look at the evidence, of the 52 active cases in Vietnam, 44 were nationals returning on special flights in the last two weeks who were taken directly off the flight into quarantine. There are less than 10 active cases contracted domestically.
Singapore – Of the 793 new cases yesterday, 791 were migrant workers living in crowded dormitories. “So I don’t think the numbers tell you much about Singapore generally. (However, the fact that a rich country like Singapore has 1.2 million foreign workers living in such impoverished conditions makes me questions the claims of Singaporean government competence…. bit like claiming antebellum southern plantations were well run.)
15. May 2020 at 17:16
@mbka
Regarding Singapore…good points. A couple of comments.
1. You jam enough people in a crowded space and the transmission rate is going to go up unless there is 100% complete immunity. I don’t think anyone is suggesting BCG vaccinations provide complete immunity. What they may do is provide some degree of immunity and resistance which may significantly lower the transmission rate all else being equal.
2. Bangladesh only achieved near universal BCG vaccination rates in the last 5 to 10 years. A significant percentage of the Bangladeshi workers in Singapore are of an age where they would not have received vaccinations.
3. India achieved universal BCG vaccinations much earlier. The case rate for Indians in Singapore is much, much lower than for Bangladeshi.
You also said, “I’m much more surprised that some of the countries with the most extreme measures, such as Italy and Spain, have not really seen more radical declines commensurate with their desperate efforts.”
Good question… and I think it leads one to hypothesize that maybe some types of government “efforts” have very little actual impact on transmission.
15. May 2020 at 18:09
Excess deaths would be the best measure of success, given that all countries are likely undercounting CV-19 deaths. And even if excess mortality captures non-Covina deaths, that is a feature, as the reaction to the virus is so extreme that it makes sense to include them in an accounting of fatality due to the pandemic.
15. May 2020 at 19:01
MikeDC, Charles
I live in Thailand. The media here is relatively free, and there is no suggestion of undercounting. I am sure there is some.
Hong Kong is a defined region, closed borders, and competent authorities can obtain results, through tracing etc.
Thailand, like the US to Mexico, has de facto porous borders to Burma, Cambodia.
People in Thailand do wear masks, and theaters have been closed etc. But no more or less, roughly, than the US.
The experience of Thailand and Vietnam may have a reason beyond simple luck.
Interestingly, the 1918 flu seemed to hit young people more than old people. Some have suggested older people had been exposed at some point to a similar virus.
But perhaps Thailand and Vietnam will get hit with “second waves.”
The problem with lockdowns is there is no exit strategy, beyond “wait for a vaccine.” Ironically, a successful lockdown results in a novel virus, which cannot be eradicated, and a still-naive population. Permanent vulnerability.
16. May 2020 at 00:15
“What can we infer from this list?”
Someone’s a nut? You really left out a bunch of European nations, I think – Finland, Serbia, Slovakia, Slovenia, maybe? Some of the others are declining pretty rapidly also, but I guess they have too many active cases still.
Throwing out a bunch of mostly insignificant countries, what you’ve really got is a bunch of European countries with a declining pandemic and a bunch of Asian countries that never really let the pandemic get started.
If Switzerland and Germany are “successful” now, shouldn’t one wonder whether they’ve really been just as “successful” all along?
16. May 2020 at 01:58
Dtoh,
re: Singapore dorms, not sure where you get your detailed knowledge of infection rates between Indian, Bangladeshi, BCG vs non BCG from… If I’d had to guess I’d say most construction workers are Bangladeshi to begin with. So they’d also have to make up the bulk of the cases. My point was rather that if BCG has any effect then it’s not very decisive.
BTW in Europe the pattern of BCG vaccination is inverse to India/Banladesh: there, it’s the older generation that received it and, not the younger ones post-80s. And yet in Europe, the older generation seems to be much more affected.
Otherwise, agreed that gov measures, even really radical ones, seem to have rather random effects. But this, if anything, reinforces Scott’s points. I’d venture that I am still not convinced that masks have a huge effect either. You get the same hit and miss pattern between countries who did / did not universally have people wear masks. E.g. Japan appears to have been late in mask adoption, so was Singapore, yet in SG the spread was never in the wider community. It seems to spread simply by close social contact, and in truly close social contact (families, canteens, dorms), people… don’t wear masks. Even if they have to wear them outdoors or in the store.
16. May 2020 at 07:25
While speculation can be useless, we all speculate. One thing we seem to never speculate about is why NYC has 1700 deaths per million and Hong Kong, Taiwan, Singapore, S.Korea, and Japan have between .5 and 5 deaths per million. I believe all these places try to count according to some predefined method—although NYC probably has the most “liberal” count. I think Richard Feynman once said (or someone thought it and said he said it) that “anyone who comments on things outside their area of expertise is as dumb as the next guy”. That sounds about right. But aren’t their “experts” in epidemiology? They don’t speculate on this either.
16. May 2020 at 09:03
Everyone, Don’t tell me country X should have been on the list; I said the list was incomplete.
Jeremy, You said:
“Active cases depends on tracking recoveries. US is not systematically tracking these.”
Agreed, which explains my comment on Noway. But the US continues to have a high rate of new cases, and some of the European countries I mentioned have also seen big declines in new cases.
You said:
“The US is high in # of deaths per million, higher than most countries, but there are definitely countries that have higher death #s per million — Sweden, UK, Italy, Spain, Frank, Belgium, Netherlands. And I think those numbers — at this point — most correctly represent how the US has done in this — worse than most but not the worst.”
No need to state the obvious in an already overlong comment.
Matt, But then what will “we see”? I made no predictions about 18 months from now, just a couple weeks.
Tuharsky, Failures can occur for reasons other than state capacity. Perhaps cultural willingness to wear masks plays a role, for instance.
dtoh, Your comments on Vietnam have no bearing on the post. As for your comparison between Singapore’s guest workers and slaves, that’s just silly. They are happy to have jobs in Singapore. I wish more East Asian countries would be similarly generous to Bangladesh. Unfortunately, as you know, many East Asian countries are quite racist and won’t let in very many dark skinned people.
And another study just came out (looking at the two Germany’s) suggesting BCG vaccines don’t matter very much. I think the vaccine may help a bit, but there are probably much more important factors.
anon, You said:
“If Switzerland and Germany are “successful” now, shouldn’t one wonder whether they’ve really been just as “successful” all along?”
Not sure of your point.
16. May 2020 at 11:21
Scott,
Regarding your comment in the interview regarding stock prices, is it not the case that lower interest rates have led to higher valuations of lower expected cash flows? Long rates have fallen significantly along with expectations for earnings and dividends (see prices of dividend futures, which go out 10 years).
Put another way, if on February 14th the S&P500 was at ~3400 based on some r (long term risk free rates plus a spread) and some g, I think at 2850 g is clearly lower now but also r is about the same since while the spread has likely gone up (as it has for corporate bonds), it’s being significantly offset by the decline of rates.
That said, I recognize that it may be bold to claim that the market’s expected return for stocks right now isn’t much higher than it was in mid-February. But if I look at the Barclays Long Corporate index, the yield to worst was 3.32% in mid-Feb and is currently at 3.55%. Granted the spread went from 141 to 248.
A DDM using dividend futures would put the current discount rate of the S&P500 at 4.75%, up from 4.55% in mid-Feb. Note as you said in the interview, the composition of the S&P500 is much more tech heavy than corporate bond indices, so therefore there’s much less distress risk being priced in.
16. May 2020 at 19:33
Scott,
I’m sure many migrant workers are happy to work in Singapore. Does that relieve the government and people of Singapore of their moral obligation to try to take better care of them especially since the cost of doing so would be minimal?
(And BTW most East Asian countries do accept large numbers of foreign workers including Japan which has significantly more Bangladeshi workers than Singapore.)
As for Vietnam, I’m merely pointing this out since your were posting “Some data on active caseloads,” and last week you admonished your readers to “[look] at the evidence from many different perspectives” in order to avoid phony data. I assumed you would appreciate the additional evidence.
16. May 2020 at 19:44
Scott, thanks!
I didn’t think it would make much of a difference in practice to buy longer bonds. Just that it’s a simple and very conventional sounding way to avoid the zero lower bound.
No need for futures or QE etc. As long as your perpetual bond has any positive value, you have a positive interest rate. And there’s no limit to how high a central bank could bid those consoles up with newly created money.
16. May 2020 at 19:53
@mbka
I haven’t looked at vaccination data closely enough to say anything definitive, but I would make a couple of points.
Many countries (Italy, U.S.) have never had vaccination programs and other countries had programs for a short number of years.
Transmission is function of (among other things) the percentage of the population which has resistance so it’s entirely possible that the effect is exponentially greater when close to 100% of the population is inoculated instead of just a limited cohort in a particular age range.
Some evidence suggests that the effect is greater for neonatal vaccination rather than later (elementary) school vaccination which may explain some of the differences.
There are multiple strains of the BCG vaccination and again some data suggest that may account for some differences between countries.
I’m not in any way suggesting the data are conclusive, but given the huge differences in mortality rates between different countries and the very strong correlation with BDG vaccinations, it’s hard to come up with a better hypothesis.
16. May 2020 at 20:12
Scott,
Regarding BCG vaccinations
East Germany discontinued vaccinations 30 years ago. And recency counts…. See
https://www.medrxiv.org/content/10.1101/2020.04.23.20077123v2 for the latest.
Abstract says….
We found a strong negative correlation between the years of BCG administration and a lower DPM [Deaths per million] along with the pandemic progression in time. The results from multivariable regression tests with 22 economical, demographic, and health-related quantitative properties for each country substantiate the dominant contribution of BCG administration years to the COVID-19 outcomes. Analyzing countries according to an age-group partition reveals that the strongest correlation is attributed to the coverage in BCG vaccination of the young population and mostly to recent years immunization. We propose that BCG immunization coverage, especially among the most recently vaccinated contributes to attenuation of the spread and severity of the COVID-19 pandemic.
And BTW – there is a significant difference in covid mortality between east and west Germany.
17. May 2020 at 01:14
Dtoh,
I’ll let a real statistician comment on that paper as surely some will. An r value below .50 isn’t as good as it sounds. If you look at the scatterplots – first thing you notice is the huge spread in DPM differential at BCG = 0 meaning that in countries that never did BCG vaccinations, you can get a massive spread of different outcomes. That alone would lead one to suspect that BCG is not a major contributor, and possibly, a proxy for something else that truly generates the correlation.
Also, until they started splitting up by age (and even then…), I wouldn’t run correlations through this kind of gunshot pattern, though it is interesting enough that yes, these correlations are all negative and significant, if generally weak. Fig 7 could be the most convincing one if not for the fact that they use 2 different non parametric tests for the two classes of vaccines they compare. This suggests that they picked whatever statistical technique from the software package that gave them the result they wanted. No justification for picking these tests is given. The rest of the paper’s approach, where they don’t use a threshold p but give the actual numerical p values where it suits them, is similarly odd as an approach. Basically not to say that it must be wrong, but, it would be nice if this thing did get its peer review.
A paper such as this, using multivariate analysis, would have been more interesting if they had done some kind of cluster analysis, instead they focus on BCG alone when they had 22 other covariates available that could have led to interesting factor combinations, or corrections.
17. May 2020 at 07:36
The following is a quote from Ryan McMaken of the Mises Institute, regarding NYC Covid deaths. (April 29)
“The real question we should be asking ourselves is why is New York is such a mess in terms of COVID-19? New York’s deaths aren’t just high by US standards. The state’s total deaths per 100,000 are higher than both Spain’s and Italy’s, both of which are considered to be among the most hard-hit countries on earth. New York has reported nearly as many COVID-19 deaths as Spain (23,500), even though Spain has a much larger population of 46 million. New York is also only about 5,000 deaths behind Italy, even though Italy has a population three times the size of New York State.
Indeed, these numbers are so high that one wonders if deaths are even being counted properly, or if there is something about New York’s medical infrastructure that is especially inferior. Perhaps New York is home to a particularly virulent strain of the disease. Perhaps the disease was in circulation for far longer than the experts insist is the case. The experts don’t know the answers to these questions.”
His two speculations. “Perhaps (NYC) has a “particularly virulent strain”. “Perhaps the disease was in circulation far longer than is thought to be the case”.
Experts don’t know the answers. But Scott does not have enough interest to discuss this topic. My speculation is the answer may be the key to the cause of the pandemic. Unfortunately, there are few speculations which are consistent with randomness.
17. May 2020 at 13:02
@Michael Rulle
I would be looking at mortality rates in NYC versus Madrid and Milan. Clearly proximity and population density are going to have an effect on the transmission rate, the incidence rate and the mortality rate. Also I think it will take time to get all the answers. Once random anti-body testing can be done and actual excess death numbers become available, we will know a lot more about actual incidence and mortality.