

Masks, not lockdowns
It’s becoming more and more obvious that we completely blew it, with a wide variety of villains (including me.)
We went for lockdowns, when the actual solution was masks, testing and voluntary social distancing. If we had done those things in early February then the death total would likely be less that 115, not 115,000. Yeah, I know this would have been politically impossible in the USA, but it still needs to be said. We blew it.
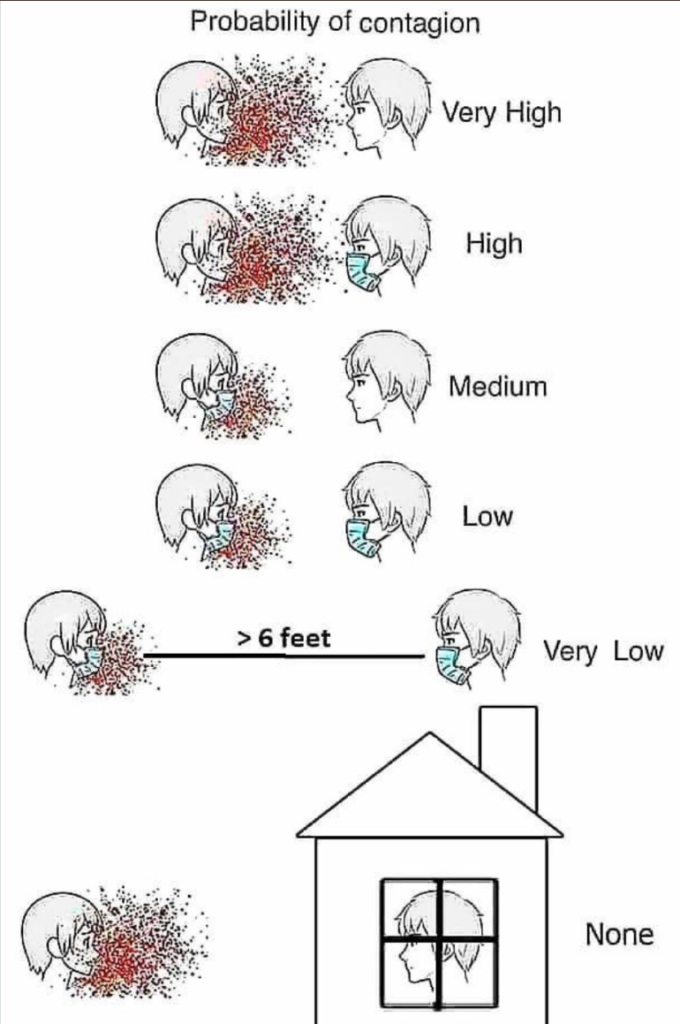
A new study suggests that masks alone will keep R0 below 1.0, if worn by just 50% of the population. If you have near 100% usage as in some East Asian countries then R0 will be far below 1.0.
The study found that if people wear masks whenever they are in public it is twice as effective at reducing the R value than if masks are only worn after symptoms appear.
In all scenarios the study looked at, routine face mask use by 50% or more of the population reduced COVID-19 spread to an R of less than 1.0, flattening future disease waves and allowing for less stringent lockdowns.
I like this graphic:
At least as recently as May, a major US manufacturer had 7 million/month in surgical mask production lines inactive, due to stupid government policies. (Probably due to price gouging restrictions.)
And what can you say about a country that doesn’t even have the police wear masks?

Americans have been spoiled for far too long.
Some claim that the BCG vaccine helps, but a new study pours cold water on that theory:
The Bacille Calmette-Guérin (BCG) tuberculosis vaccine has immunity benefits against respiratory infections. Accordingly, it has been hypothesized that it may have a protective effect against COVID-19. 12 randomized controlled trials are currently underway to test this hypothesis, but their results shall not be available before at least five months. Instead, this paper uses a nationwide natural experiment. In April 1975, Sweden discontinued newborns BCG vaccination. The vaccination rate fell from 92% to 2%. I compare the numbers of COVID-19 cases and hospitalizations for cohorts born just before and just after that change. I find no statistically significant differences, and I can reject small BCG effects. Thus, receiving the BCG vaccine at birth does not seem to have a protective effect against COVID-19.
Again, masks, testing and voluntary social distancing (including no hand shaking). Do that and we can avoid a second wave this winter. But I doubt we will.
HT: Razib Khan
Tags:
12. June 2020 at 10:43
Maybe it was impossible, but the effort to message mask wearing, social distancing, and “safe operation of public spaces as a civic duty to others was not tried.
12. June 2020 at 12:49
Data on BCG vaccination as a protective measure against SARS-CoV-2 are all over the map. There are 14 trials world wide including the US to see if it does offer protection. I’m not optimistic that it will work given all the papers I have read but unlike the referenced paper above which is also inconclusive, I won’t rule out a slight effect.
12. June 2020 at 13:36
Alan, I agree that there may be a small effect, indeed I still think it’s likely there’s a small beneficial effect.
12. June 2020 at 13:46
Scott,
The BCG study has serious defects and adds nothing new to our understanding of the effect of BCG vaccinations on the Covid pandemic. … not surprising given that the author is an economist with no background in epidemiology.
All of the previous studies on the subject confirm that the vaccination does not provide lifetime immunity. (It doesn’t even do that for TB.) None of the studies would claim that the vaccination provides a significant protective effect to individuals who received it 45 years ago (as is the case in Swedish study you have cited.)
All of the studies hypothesize that the benefit of the vaccination comes from providing immunity to more recently vaccinated (i.e. younger) individuals thereby reducing overall community (R0) to below 1. Nothing in the study refutes that.
The study relies on a discontinuity in vaccinations in 1975 in Sweden and looks at covid incidence in cohorts aged just below and just above the age of 45. The study recognizes that 25% of the Swedish population are immigrants, but fails to normalize for the fact that covid incidence is much higher (3 to 5 times as high) in the immigrant population where there is no known discontinuity in the BCG vaccinations in those age cohorts.
Scott, you should at least read the studies before you cite them. The whole study is a 3 minute read and that’s all the time it takes to realize the thing is meaningless.
12. June 2020 at 13:56
Sumner has been watching too many of those disaster movies where the hero runs around telling people what to do, with some simple solution like “get out now!!!” but nobody will listen to them. That’s Sumner here: Covid-19 magically goes away if all people wear masks, according to a non-peer reviewed study. Yet Sumner makes this howler: “If we had done those things in early February then the death total would likely be less that 115, not 115,000.” -LOL! 115? not 116? R U shur perfesser? And despite the non-peer reviewed Harvard medical paper the other day saying the Wuhan flu virus was widely circulating in Wuhan in August of 2019, based on Baidu/Google searches and satellite images of hospital parking lots? Seriously? Who’s paying Sumner to spread this propaganda?
I do agree however that lockdowns have a cost, and unless religiously followed, like in Wuhan (apparently), certain Asian countries, Greece, they are unlikely to work. So for the undisciplined USA, lockdowns likely won’t work and a second wave is inevitable.
Covid-19: the Coast is Toast! Coming to a crowded theatre near you this fall…
12. June 2020 at 14:53
Scott,
you were right, once again. Masks are effective, and together with distancing and testing, any country can get a good grip on the disease.
We wouldn’t even (desperately) need a vaccine, if only these rules were followed everywhere.
With these rules, the disease can even be eradicated, as Australia and New Zealand are just proving.
I was also sceptical about masks in the beginning because I was afraid that people would become less careful. My personal experience is now the opposite, and it makes sense: people who wear masks behave more cautiously, oftentimes way more cautiously, than those who still refuse to wear masks.
As far as I understand the topic of BCG, it may just reduce the severity of the disease a tiny bit, if at all. So BCG would not be helpful if we want to stop the spread of the disease. In any case, the effect so far is too small to justify the use of the drug. A new genetically modified BCG vaccine has been developed in Germany, which is supposed to have very few side effects, and yet it is not used because there is still no final proof whatsoever that BCG has a relevant effect against corona.
12. June 2020 at 15:43
No nation has yet had a second wave.
Policy must be made with a realistic assessment of domestic populations. Americans are what they are.
Also, the US seems to decentralize certain health policies down to state and local levels, such as mask-wearing or business restrictions. And there is a de facto open border with Mexico.
I think Sumner is right— the US will suffocate the economy but the health benefits will be dubious. We may see more social unrest.
12. June 2020 at 21:03
There is significant evidence that live vaccines boost trained immunity (altering the epigenetics of the innate immune system mainly). BCG is one of these live vaccines (also measles and oral polio). However, in the 45+ years that these vaccines were administered it is possible many other epigenetic changes have happened (not to mention immune senescence post-65 years old!). So, it is hard to see how vaccines delivered 45+ years ago not working is necessarily pouring cold water on the idea.
12. June 2020 at 23:37
Great, another mathematical model “proving” cloth masks work even though the authors didn’t differentiate those from surgical masks in
their models. Again, a few years ago a study among health workers showed cloth masks stop 3% of a virus compared to 44% for surgical masks.
Also, a yougov survey taken in February shows 90% used masks in Taiwan, Hong Kong and China but only 66% in Japan. Despite that, Japan and South Korea have ended with about the same number of Covid 19 deaths per capita: Japan 920 deaths, South Korea 277 deaths so
Japan…….0.0000072
S. Korea….0.0000054
U.S………0.00035 and not over this round
That’s 50 times as many U.S. deaths per capita as Japan so far.
13. June 2020 at 03:33
Scott,
for the past 2 1/2 months, Singapore had mandatory masks, mandatory distancing: Most businesses closed, those open must follow strict physical distance requirements between patrons, capacity limits at 1 person per 16 sq m (about 170 sq ft), tracing of anybody entering any shop or office with mandatory apps, massive testing, and immediate isolation of anybody testing positive. In short, Singapore is doing what is humanely possible.
The result: ca. 40,000 infected, 29,000 recovered, 11,000 still active cases, of which less than 300 (!) in hospital and just 2 (!!) in intensive care. 25 deaths total since January. The infections in the foreign worker dorms continue at a rate of about 300-500 new ones per day in spite of the most minute safety protocols in those dorms, including distancing, staggered meal hours, masking, and separating out of cases vs healthy pax and testing on a massive scale for the past 2 months. Community numbers are also slowly creeping up since the lockdown was gradually eased 10 days ago. Mind you, still no retail and no restaurants! Still masks! Still only family visits 2 pax at a time! Still only 20% of office workers back at office; in our office no more than 4 workers at a time etc. – yet number are slowly creeping up even outside dorms.
No matter what pet hypothesis you’re entertaining: masks, BCG (mandatory in SG), polio vaccine (mandatory in SG), social distancing, testing, isolating cases early, death rate theories of whatever kind … I challenge you to explain what’s happening in Singapore. Personally, I am inclined to throw up my hands in the air and just say, I have no idea. I liked your post “nobody knows anything”, that’s about it for me.
13. June 2020 at 08:57
Mbka:
Your numbers indicate 25 deaths for a minimum 40,000 infections.
That is one death per 1,600 reported infections.
Amazing result…I assume only dorm workers are getting infected….younger population
13. June 2020 at 09:34
Benjamin,
here’s the data. About 1800 community residents and 38,000-ish dorm residents.
https://www.straitstimes.com/multimedia/graphics/2020/02/spore-virus-cases/index.html?shell
13. June 2020 at 09:56
dtoh, Your explanation seems so implausible that it actually makes me less likely to believe the theory. It’s only useful for the young? But almost everyone dying is old! And we know that Covid-19 will run like wildfire through even a population that has universal BCG if nothing is done to stop it. Look at Wuhan. Look at that religious cult in South Korea.
Tony, I’m not saying that administering the vaccine now is a bad idea, I’m addressing the claim that countries that have always administered it have low current death rates because their old people got an inoculation 60 years ago.
I find the claim that it would help today for everyone to get a BCG shot to be a highly plausible theory, albeit unproven. But that’s not the theory I was addressing.
Todd, Then wear surgical masks! That’s what I do.
The rest of your comment keeps repeating the mistake of assuming only one factor matters. How many times do I need to say that multiple factors matter. Read Christian–he gets it.
And why say Japan has “only” 66% usage, after the study says 50% is enough to keep R0 below 1.0? What’s your point?
mbka, Well we both agree that Singapore has succeeded in keeping the death rate super low, which is what matters. So let’s start with the fact that Singapore is a huge success story.
Then we agree that it’s now almost 100% a dorm problem. I don’t know as much about the dorm situation as you do, but obviously the Singapore story is almost 100% explained by different conditions in the worker dorms vs. outside the dorms. What differences are crucial, I don’t know. Density? Behavior? Ventilation?
13. June 2020 at 10:29
Mask wearing definitely seems to be a key component to reduce/eliminate COVID spread. Unfortunately, for some reason wearing a mask – which is barely an inconvenience – has become severely politicized.
13. June 2020 at 13:59
Scott,
You said, “And why say Japan has “only” 66% usage, after the study says 50% is enough to keep R0 below 1.0? What’s your point?”
Gosh read your own advice, “How many times do I need to say that multiple factors matter.”
Without masks the RO is going to be different in different places so no way will the amount of mask wearing required to get R0 below is going to be exactly 50% regardless in every location. Different factors exist in different locations. It’s obviously going to be a lot lower than 50% in rural North Dakota (probably not required at all) and a lot higher in densely populated urban areas. It depends on the number and type of social interactions that occur.
As I have said many times, it’s hard to imagine that with 15 million unmasked daily subway riders in Tokyo, that you would not have had a high level of transmission if all else were equal.
13. June 2020 at 15:15
Scott,
Regarding BCG….to me it seems obvious, but to make it clear..
1. There is only data on confirmed cases of Covid.
2. Nobody yet knows with any certainty what is the number of actual cases because of differences in the rate of testing and because they don’t know what is the percentage of asymptomatic cases.
3. Accordingly, know one knows for sure what is the actual case fatality rate.
4. What is known with some certainly is the overall fatality rate in the population.
5. Everyone agrees that there is a strong negative correlation between the overall fatality rate and BCG vaccinations. The only thing that is being debated in causality.
6. Immunity is not binary. Specific immunity may be, but general immunity is not.
7. General immunity lowers the risk of infection, but doesn’t eliminate it. If you put someone with a high level of general immunity in crowded dormitory or church choir, they can still contract the disease.
8. I think most people believe that BCG does not provide specific immunity but rather increases a person’s general immunity with that effect decreasing over time.
9. In order to reduce Covid (and associated mortality) in a population, all that is required is a reduction in transmission.
10. Any higher level of immunity in any fraction of the population will reduce transmission. In the extreme case, the difference between R0>1 and RO<1, could be one individual with a slight increase in general immunity.
11. Countries with BCG vaccinations have seen a significant decrease in Covid mortality (50X in the case of Japan.) This suggests that there is a significant level of immunity conveyed to a significant portion of the population.
12. Sweden on the other hand has a much smaller portion of the population that has been vaccinated and the amount of time elapsed since they were vaccinated is known to result in a significant decrease in immunity conferred. Thus the impact on transmission (and Covid associated mortality) is likely to be minimal.
13. Whether the BCG vaccination reduces morbidity or mortality in people who contract the disease is unclear. Data from the Diamond Princess suggest it does, but I don't think there is yet sufficient data to substantiate this.
14. If the vaccination does reduce morbidity, it is also possible that a reduction in viral load or symptoms like coughing could further reduce transmission.
13. June 2020 at 17:11
Am I the only person who is frustrated that there is not an authoritative source on what the most effective mask is? And what the strengths and weaknesses of different designs are? That seems like something the CDC should be able to provide fairly easily?
13. June 2020 at 18:52
The CDC is apparently incapable of doing anything except for slowing things down and getting the IFR horribly wrong with no supporting evidence
14. June 2020 at 02:58
“The rest of your comment keeps repeating the mistake of assuming only one factor matters. How many times do I need to say that multiple factors matter. Read Christian–he gets it.”
No, Mr. List doesn’t get this one bit. There may be multiple reasons except we have a fairly recent study that cloth masks are worthless and give a false sense of security and even surgical masks prevent only about 50% of the virus from being inhaled. That may be helpful but not at all obvious.
We also have good clues from two recent studies that 1) Norway’s lockdown was not effective and that they would have been better off following Sweden, although Norway has better nursing homes prior to the outbreak. 2) Government policies, such as lockdowns, have had minimal effect on outcomes but instead prior initial conditions have determined outcomes.
Australians hardly used masks since the government recommended that they not be used yet have had about 100 deaths or on the order of about 100 times fewer deaths than the U.S.
Japan had the lowest mask use for February at 66% in Asia that I saw at the Yougov site. With the rest over 70% and China, Taiwan and Hong Kong at 90%. Maybe 66% made a difference – I don’t know – but masks sure didn’t make a difference in Australia.
The New Zealand government only started to think about masks in May, several weeks after coronavirus entered the country. From May 7: A high-level scientific review has explored the vexed issue of face masks – finding there’s not enough evidence to recommend people wear them to protect against Covid-19.”
14. June 2020 at 06:36
Scott,
my point was about the fact that Singapore made every effort in the book to contain the dorm problem, yet success is coming very slowly. The dorm situation arose and continues to exist, nearly 2 1/2 months after universal mask compulsion, closure of the most affected dorms, spreading out of workers into a host of facilities etc. Workers continue to get infected in spite of masks, youth, recent BCG (presumably), distancing efforts, testing, immediate isolation of the infected etc. I tend to think a mix between your earlier “nobody knows anything” post and what Todd said above – much has to do with initial conditions. And I also see it differently now in the light of the other article I liked to a few days ago on clustering. This article compared Covid outbreaks to a fire that emits a lot of embers. Most actually go out (most people don’t infect anyone) but once a cluster forms (a new fire) it is very hard to get rid of it. Masks or otherwise. And community infections are also creeping back up in SG even though now masks are compulsory, which they weren’t in February when numbers also crept up. The low death rate could be a result of the youth of the dorm workers, although really they’re likely 25-40. No teenagers there. They’re construction workers after all. But then again why do these youngish people get infected so readily in the first place? I can’t get my head around any of this and I am still not sold on universal masks.
14. June 2020 at 06:41
Is Canada similarly dysfunctional? A country of 38 million people has reported 8,107 deaths (215 dead per million).
The COVID capital of the world of course is the US northeast (New York, New Jersey, Connecticut, Massachusetts, Rhode Island), a contiguous area with 40 million people and 56,165 COVID deaths (1,407 deaths per million, leaving Belgium in the dust).
Outside here, the rest of the USA has 292 million people and 59,506 COVID deaths. 204 deaths per million, a smidgen better than Canada.
I haven’t seen it laid out like this in the media. Instead, we here how things are winding down in the hard hit states and growing in the icky irresponsible Red states. And yet, the northeastern states mentioned above continue to contribute 25%-30% of total new deaths, despite comprising only 12% of the population.
The northeast horror show is vastly underappreciated.
14. June 2020 at 08:43
Justin, Yes, that’s sad.
dtoh, The initial (severe) outbreak in Wuhan occurred in a country with BCG vaccine. I can believe it might have been worse in Wuhan without the BCG, but surely not 10 times worse!
I don’t know why Tokyo was hit much less hard than Wuhan, but it seems implausible that Tokyo’s success can be explained by the BCG vaccine. (Yes, other factors matter, but Tokyo is no warmer than Wuhan, or less crowded, etc. And the problem is now getting worse in the southern US, even as it gets warmer.)
As for the correlations, I wonder if the studies have taken into account the newest data. Right now South America is getting hammered while Australia and NZ do very well. And yet South America has a much higher rate of vaccination. Similarly, early studies tried to explain Italy by their vaccination policy, but now Spain and the UK are hit harder despite having more vaccinations. This isn’t over, we’ll need more studies.
BTW, if there’s even a 20% chance you are right about a 10X effect, then Bill Gates should be building BCG vaccine factories right now. (I expect NOTHING from our government.) Even a 20% chance you are right means the vaccine would be worth a trillion dollars in social welfare.
mbka, Isn’t the most likely explanation that they are getting infected in the dorms? If the migrant workers were getting infected while out shopping or walking around, then why wouldn’t local Singaporeans also be getting infected in large numbers?
Maybe it’s something simple, maybe they disobey mask wearing requirements once inside the dorm, as they find them cumbersome.
BTW, 25-40 year olds have a very low Covid death rate in most countries.
Brian, I don’t get your comparison. Most of the problem in Canada is Quebec. Why exclude the Northeast US but not Quebec? That makes no sense to me.
Also note that colder parts of the US were initially hit much harder than warmer parts, and Canada is even colder than the northern US.
14. June 2020 at 10:41
Scott: “Right now South America is getting hammered”
Brazil’s deaths are increasing at 2.5% a day, down from 6% a day in the first half of May. Argentina is a little over 3% a day but only 820 deaths compared to 43,000 covid-19 deaths in Brazil. If Argentina was as large as Brazil then 3,800 deaths. Why is Brazil doing 10 times worse as Argentina? Perhaps mask usage…or not.
14. June 2020 at 16:34
I cannot say I told you so because I did not. But, for myself at least, I have leaned this way (but agreed reluctantly with the initial shutdown—-big error) but as time has passed beginning in the first few weeks I struggled with trying to understand what was bothering me. I want to explain what I began to believe a few weeks ago.
This is at best a hypothesis and at worst a reasonable speculation. We will find out eventually how accurate it is. We know with certainty this is a disease of the old. We know that the median age of deaths are in the high 70s to low 80s. Keeping it simple so I don’t write forever—very few people under 65 die. Less than flu. People who die are dying at an age when people die. This implies (maybe there is another reason) the disease is not that strong as it only kills people who might be dying anyway. Because we define “dying of Covid as having Covid” it is easy to conflate. If the disease were a true severe killer younger people would die at a much higher rate. New York City, an outlier, still has only 8% of deaths under 65. Stated in the most extreme way possible ( just to make the directional point) death by Covid has been a partial illusion. When we ultimately ( if ever, but maybe in a few years) find out the real numbers by discovering “extra deaths” we will know. Of course Covid kills and it is bad. But it has been exaggerated—-and the economic effects at least counteract it. I am expressing this very simply to make the point. One piece of evidence, if you will, is daily cases in last 2 months have been up 80%, but daily deaths down about about 50% world wide. Not proof but consistent with hypothesis as we test more young
14. June 2020 at 17:25
Scott,
“I can believe it might have been worse in Wuhan without the BCG, but surely not 10 times worse!”
Covid fatalities were 7.5 times higher in NYC than in Wuhan.
Also not to get into the weeds, but researchers are finding a correlation between the specific strain of BCG used in vaccinations and the transmission rate in the population. China uses a “weaker” strain than Japan or Taiwan.
15. June 2020 at 05:33
For the period 2/1/20-6/6/20 total excess deaths (as of 6/12/20) in US is 45,000. Excluding NYS it is almost zero. There are delays in reporting so this is understated. The CDC does not provide death numbers for those who died only with COVID. They do provide deaths from those who Had Covid and other diseases.
April had very high excess deaths——-dominated by N.Y. and NJ.
15. June 2020 at 06:37
Scott,
I cited relevant facts WITHIN the United States to point out how the media continues to distort what is going on.
In mathematical terms, they are citing large % increases from low baseline numbers, failing to understand that low % increases from high baseline numbers produce more corpses.
At some point, the rest of the US will start contributing deaths in proportion to their population (I mean, they have to given the current case numbers, right?), but the trajectory here is not close to what the NE went through in March.
As far as Canada, yeah, there is definitely an element of weather here, but it’s obviously not decisive. When I talk about the COVID capital of the world (NY, NJ, CT, MA, RI), it’s really the tiny strip of land along the coast where most of the carnage has taken place. Upstate NY and Western Massachusetts not hit so hard, while NH less so, and Vermont and Maine, which are entirely buffered from the coast have done very well despite their latitude.
All of this land sits between the US NE coast and the Canadian hotspots you identified.
There are actually lots of interesting stories here, but you have to look harder than the media is capable of or interested in.
For example, can I direct your attention to Wisconsin? Among midwestern states, it had a high death toll early, but then they did something (Remember the Wisconsin election doom-mongering? Nobody else does.)
Michigan and Illinois hit hard, and Indiana less so. Minnesota looked fine but at some point it looks like they decided to go Sweden. Iowa ended up suffering a bleed from Illinois and Minnesota.
Meanwhile, Wisconsin’s numbers look like… Germany’s, except they’re surrounded by a bunch of states doing much worse.
You are familiar with both of these geographical areas (upper midwest and NE). I’m sure if you took an interest, these stories would pop out at you.